Fill a Valid California Dmv Dl 546 Form
In the State of California, the Department of Motor Vehicles (DMV) mandates that individuals seeking or holding a driver's license may be required to fill out a Health Questionnaire, known as Form DL 546, to ensure they meet the medical qualifications necessary for safe driving. This form serves as a critical tool in assessing the health and physical abilities of drivers, thereby directly affecting public safety on the roads. Applicants are instructed to answer a series of questions that cover a wide range of health issues, including but not limited to vision and hearing impairments, diabetes management, cardiovascular health, and neurological conditions. The DL 546 form is designed to identify any physical or mental conditions that could impair an individual's ability to operate a vehicle reliably. By stipulating that "yes" answers may necessitate a more detailed examination or consultation with a physician, the DMV aims to foster an environment where only those fit to drive, in the healthiest capacity, are granted that privilege. Importantly, this process underlines the DMV's commitment to reducing traffic accidents linked to medical conditions. Furthermore, the requirement for submitting this form every two years reinforces the ongoing assessment of a driver's health status, ensuring that any new or existing conditions are adequately managed and do not pose a risk to the safety of the driver or the public.
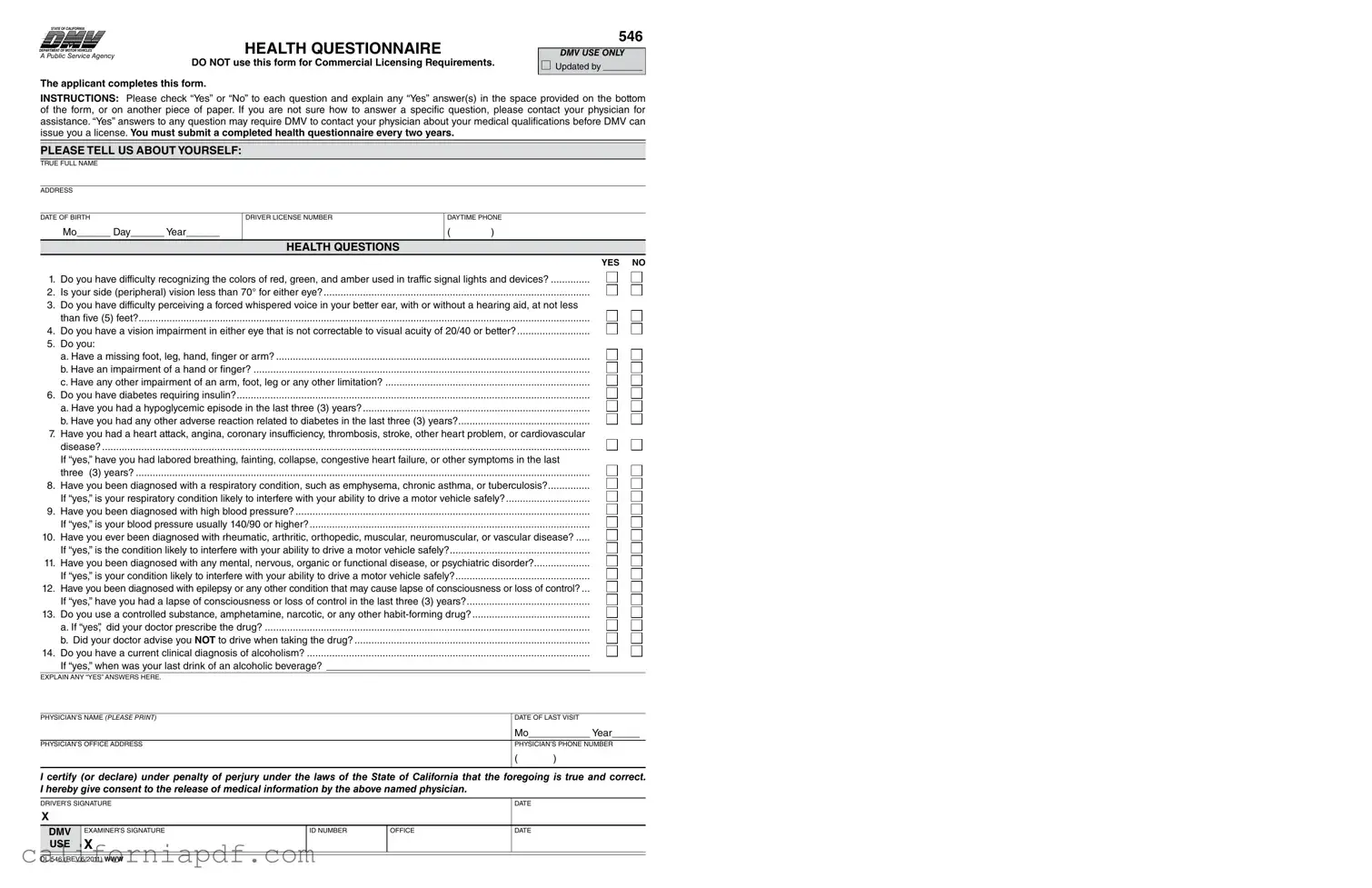
Document Example
STATE OF CALIFORNIA
DEPARTMENT OF MOTOR VEHICLES®
A Public Service Agency
HEALTH QUESTIONNAIRE
DO NOT use this form for Commercial Licensing Requirements.
546
DMV USE ONLY
updated by ________
The applicant completes this form.
INSTRUCTIONS: Please check “yes” or “no” to each question and explain any “yes” answer(s) in the space provided on the bottom of the form, or on another piece of paper. if you are not sure how to answer a speciic question, please contact your physician for assistance. “yes” answers to any question may require dmv to contact your physician about your medical qualiications before dmv can issue you a license. You must submit a completed health questionnaire every two years.
PLEASE TELL US ABOUT YOURSELF:
true full name
address
date of birth
mo______ day______ year______
driver license number
daytime Phone
()
|
HEALTH QUESTIONS |
|
YES NO |
1. |
do you have difficulty recognizing the colors of red, green, and amber used in traffic signal lights and devices? |
2. |
is your side (peripheral) vision less than 70° for either eye? |
3. |
do you have difficulty perceiving a forced whispered voice in your better ear, with or without a hearing aid, at not less |
|
than ive (5) feet? |
4. |
do you have a vision impairment in either eye that is not correctable to visual acuity of 20/40 or better? |
5. |
do you: |
|
a. have a missing foot, leg, hand, inger or arm? |
|
b. have an impairment of a hand or inger? |
|
c. have any other impairment of an arm, foot, leg or any other limitation? |
6. |
do you have diabetes requiring insulin? |
|
a. have you had a hypoglycemic episode in the last three (3) years? |
|
b. have you had any other adverse reaction related to diabetes in the last three (3) years? |
7. |
have you had a heart attack, angina, coronary insufficiency, thrombosis, stroke, other heart problem, or cardiovascular |
|
disease? |
|
if “yes,” have you had labored breathing, fainting, collapse, congestive heart failure, or other symptoms in the last |
|
three (3) years? |
8. |
have you been diagnosed with a respiratory condition, such as emphysema, chronic asthma, or tuberculosis? |
|
if “yes,” is your respiratory condition likely to interfere with your ability to drive a motor vehicle safely? |
9. |
have you been diagnosed with high blood pressure? |
|
if “yes,” is your blood pressure usually 140/90 or higher? |
10. |
have you ever been diagnosed with rheumatic, arthritic, orthopedic, muscular, neuromuscular, or vascular disease? |
|
if “yes,” is the condition likely to interfere with your ability to drive a motor vehicle safely? |
11. |
have you been diagnosed with any mental, nervous, organic or functional disease, or psychiatric disorder? |
|
if “yes,” is your condition likely to interfere with your ability to drive a motor vehicle safely? |
12. |
have you been diagnosed with epilepsy or any other condition that may cause lapse of consciousness or loss of control? ... |
|
if “yes,” have you had a lapse of consciousness or loss of control in the last three (3) years? |
13. |
do you use a controlled substance, amphetamine, narcotic, or any other |
|
a. if “yes”, did your doctor prescribe the drug? |
|
b. did your doctor advise you NOT to drive when taking the drug? |
14. |
do you have a current clinical diagnosis of alcoholism? |
|
if “yes,” when was your last drink of an alcoholic beverage? _______________________________________________ |
exPlain any “yes” answers here.
Physician’s name (PLEASE PRINT) |
date of last visit |
|
mo___________ year_____ |
|
|
|
|
Physician’s office address |
Physician’s Phone number |
|
|
( |
) |
I certify (or declare) under penalty of perjury under the laws of the State of California that the foregoing is true and correct. I hereby give consent to the release of medical information by the above named physician.
driver’s siGnature |
|
|
date |
|
X |
|
|
|
|
|
|
|
|
|
DMV |
examiner’s siGnature |
id number |
office |
date |
USE |
X |
|
|
|
|
|
|
|
|
dl 546 (rev.6/2011) WWW
Form Breakdown
| Fact Name | Description |
|---|---|
| Form Purpose | The DL 546 form is a health questionnaire used by the California Department of Motor Vehicles to evaluate a driver's medical qualifications for a non-commercial driver's license. |
| Submission Requirements | Applicants must submit a completed health questionnaire to the DMV every two years to maintain their driving privileges. |
| Content of Form | The form includes questions about the applicant's ability to recognize traffic signal colors, peripheral vision, hearing, vision impairments, physical impairments, and health conditions that could affect driving ability. |
| Governing Law | The DL 546 form is governed by the laws of the State of California, specifically under the jurisdiction of the California Department of Motor Vehicles (DMV). |
| Physician Involvement | "Yes" answers to any question may require the DMV to contact the applicant's physician for more information about the applicant's medical qualifications for driving. |
How to Write California Dmv Dl 546
Filling out the California DMV DL 546 form is a crucial step for individuals seeking to ensure their eligibility to operate a motor vehicle safely, in compliance with state regulations. This form is designed to assess the health and physical abilities of the driver. Carefully and truthfully completing this form is essential as it helps the Department of Motor Vehicles (DMV) make informed decisions regarding one’s driving privileges. Here are step-by-step instructions to assist you in filling out the form accurately:
- Begin with the section titled "PLEASE TELL US ABOUT YOURSELF." Enter your true full name, ensuring it matches the name on your official identification documents.
- Provide your address in the space given. This should be your current residential address.
- Fill in your date of birth, using the format month (mo), day, and year (year).
- Enter your driver license number in the designated area. If you have a current license, this information can be found on it.
- Provide a daytime phone number where you can be reached. Include the area code.
- Proceed to the "HEALTH QUESTions" section. For each statement, check either "yes" or "no" based on your personal health condition and circumstances.
- If you answer "yes" to any questions, you must explain your "yes" responses in the space provided at the bottom of the form or on a separate piece of paper. Be clear and provide sufficient detail regarding your condition.
- If unsure about how to answer any specific question, it's recommended to consult with your physician for accurate information.
- Underneath the health questions, if applicable, provide the physician’s name, the date of last visit (month and year), the physician's office address, and the physician's phone number.
- Read the certification statement carefully, then sign and date the form in the spaces provided for the driver's signature and date.
- Remember that this is a legally binding document. Your signature certifies that all information provided on the form is true and correct to the best of your knowledge.
- Once the form is completed, review all information for accuracy and completeness before submission.
After the form is fully completed, it should be submitted to the appropriate office as instructed by your local DMV. It’s crucial to ensure that the form reaches the designated office for processing. Timely submission and accurate completion of the DL 546 form play a vital role in maintaining or obtaining your driving privileges. The information you provide will be evaluated to determine if any further medical examination or information is necessary for the DMV to make a decision regarding your ability to safely operate a motor vehicle. Always keep a copy of the completed form for your records.
Listed Questions and Answers
What is the California DMV DL 546 form?
The California DMV DL 546 form is a Health Questionnaire that must be completed by applicants seeking to obtain or renew a driver’s license. It is used by the Department of Motor Vehicles to assess an applicant's medical qualifications for operating a vehicle safely. This form is not applicable for Commercial Licensing requirements.
Who needs to fill out the DL 546 form?
Any person applying for or renewing a California driver’s license must fill out the DL 546 form as part of the evaluation process to determine their medical fitness to drive.
How often do I need to submit the DL 546 form?
A completed health questionnaire is required every two years, ensuring the DMV has up-to-date information on your health status and driving capability.
How do I answer the health questions on the form?
For each question on the DL 546 form, check either "yes" or "no." If you answer “yes” to any question, provide an explanation in the space allocated at the bottom of the form or on a separate piece of paper. If uncertain about how to answer, consulting with your physician is advisable.
What if I answer “yes” to any of the questions?
Answering “yes” to any question requires additional action, as the DMV may need to contact your physician to discuss your medical qualifications before issuing a license. It is critical to provide detailed explanations for any "yes" responses, including dates and relevant medical details.
What happens if I do not fill out the DL 546 form?
Failing to complete the DL 546 form could result in delays in the processing of your driver’s license application or renewal. The DMV needs this information to ensure all drivers on the road meet the medical standards for safe driving.
Can I fill out the DL 546 form online?
As of the current guidance, the DL 546 form must be filled out manually. After completion, it should be submitted in person or as directed by the local DMV office. Always check the latest DMV guidelines, as processes may change.
Where can I find a copy of the DL 546 form?
A copy of the DL 546 form can be obtained from the California Department of Motor Vehicles (DMV) website or by visiting a local DMV office.
What should I do if I have more questions about filling out the DL 546 form?
If you have further questions regarding the DL 546 form, the best course of action is to contact the California DMV directly through their official website or by reaching out to a customer service representative. They can provide the most current information and guidance specific to your individual situation.
Common mistakes
When people fill out the California DMV DL 546 form, which is a health questionnaire required for driver’s license issuance, several common mistakes can potentially delay or impact the process. Being aware of these mistakes helps in ensuring that the process goes smoothly and efficiently.
- Not providing explanations for "yes" answers: The form asks for an explanation of any "yes" answers. Omitting these explanations can lead to delays, as the DMV might require additional information to assess medical qualifications.
- Incomplete personal information: Failure to complete the section that asks for personal details such as the true full name, address, and date of birth can cause the application to be delayed or not processed.
- Skipping the physician’s details: Not including the physician's name, address, and phone number, especially when "yes" answers are provided, makes it difficult for the DMV to verify health information if needed.
- Not describing the condition accurately: Vague explanations about health conditions might not provide the DMV with enough information to make an informed decision regarding driving capabilities.
- Ignoring the need for additional sheets: If the space provided on the form is insufficient, applicants sometimes fail to use an additional piece of paper for their explanations, as instructed. This might lead to missing crucial information.
- Forgetting to re-submit the form for renewals: Since the form must be submitted every two years, some individuals forget to re-submit it, which can result in license expiration and legal issues.
- Incorrectly answering questions about drug and alcohol use: Misunderstanding or not being honest about the use of controlled substances, amphetamines, narcotics, or habit-forming drugs can lead to serious legal and safety issues. This includes failing to accurately report whether these substances were legally prescribed and if there’s advice against driving while taking them.
Thoroughly reviewing the California DMV DL 546 form and carefully providing accurate and complete information ensures that the assessment process by the DMV is straightforward. This careful attention helps in facilitating a smoother process for obtaining or renewing a driver’s license, contributing to the wider goal of maintaining safe roads for everyone.
Documents used along the form
When completing the California Department of Motor Vehicles (DMV) DL 546 Health Questionnaire, it's often necessary to provide additional documents to support the information provided. Whether for initial licensing or for periodic updates required by the DMV, these supplemental forms help ensure the comprehensive assessment of an applicant's ability to safely operate a vehicle.
- DL 62 - Vision Examination Form: Used by an optometrist or ophthalmologist to report the results of a comprehensive vision test, including clarity of vision, field of vision, and ability to recognize colors.
- DL 51 - Medical Examination Report: A detailed form completed by a licensed physician to certify the applicant's medical fitness for driving, including any conditions that might impair driving abilities.
- DL 44 - Driver License or Identification Card Application: Required for new applicants or existing licensees seeking to renew or replace their driver's license, often accompanied by the health questionnaire to update personal and medical information.
- DL 939 - Verification of Vehicle Insurance: Although not directly related to medical conditions, this form verifies that the applicant has the required insurance coverage for vehicle registration or license issuance.
- DS 326 - Driver Medical Evaluation: A more in-depth medical evaluation form filled out by a physician when specific medical conditions, such as cardiovascular diseases or neurological disorders, need to be assessed in detail.
- DL 120 - Senior Driver Request for Reexamination: For drivers who are 70 years of age or older, this form can be submitted by concerned family members or physicians who question the senior’s ability to drive safely.
- DL 23 - Traffic Accident Report: In cases where a driver's medical condition may have contributed to a traffic accident, this form offers a detailed account of the incident for review by the DMPS.
Gathering the correct documents is an essential step in ensuring that all drivers on the road are capable and healthy enough to do so safely. Each form serves its unique purpose, from detailing an individual's vision capabilities to elaborating on more complex medical conditions. These forms, used in conjunction with the DL 546, help the California DMV make informed decisions regarding licensing and contribute to safer roadways for everyone.
Similar forms
The California Department of Motor Vehicles (DMV) Health Questionnaire (DL 546 form) bears a close resemblance to the Federal Motor Carrier Safety Administration (FMCSA) Medical Examination Report Form for Commercial Driver License (CDL) applicants. Both documents are required to assess the physical and mental health of drivers to ensure they are capable of safely operating a vehicle. They cover similar health concerns, such as vision and hearing impairments, diabetes, cardiovascular conditions, and neurological disorders. Furthermore, they require disclosure of any medications that might impair driving abilities. The main difference lies in their target audience, with the FMCSA form specifically focused on commercial drivers.
Another document similar to the DL 546 form is the Disability Parking Placard Application used in many states. This application assesses an individual's physical disabilities to determine eligibility for special parking privileges. Like the DL 546, it inquires about impairments that may affect one's ability to walk or travel safely, including neurological, orthopedic, and cardiovascular conditions. Both require a healthcare professional's certification, though the parking placard application specifically focuses on mobility issues rather than the broader scope of driving abilities.
The Pilot's Medical Certificate application process administered by the Federal Aviation Administration (FAA) also shares similarities with the DL 546 form. Both processes evaluate the physical and mental fitness required for operating a vehicle, in this case, an aircraft. They examine vision, hearing, neurological health, and potential substance abuse issues to prevent accidents caused by physical incapacitations. Although the standards and specific health concerns vary slightly due to the different responsibilities of driving and flying, the fundamental goal of ensuring the safety of the operator and the public is a common thread.
Lastly, the Sports Physical Examination form, required for participation in school or community sports, parallels the DL 546 form in several ways. It assesses overall health, looking for any conditions that might pose a risk during physical activity, including heart problems, respiratory conditions, and seizures, similar to the DL 546's screening for conditions that could impair safe driving. While the sports physical focuses more on physical performance and the ability to engage in sports activities, both types of evaluations aim to identify any health issues that could lead to emergencies or a loss of control in their respective activities.
Dos and Don'ts
When it comes to navigating the complexities of filling out the California Department of Motor Vehicles (DMV) DL 546 form, a Health Questionnaire, there are some crucial dos and don'ts that can streamline the process and ensure compliance. This form, which is a pivotal part of maintaining or obtaining your driving privileges, demands careful attention to detail. Here's a guiding light on how to tackle this form with precision and accuracy.
Things You Should Do:
Read the instructions carefully before you start filling out the form. This ensures that you understand what information is required and how to properly provide it.
Answer each question truthfully. The DMV requires accurate information about your health to determine your fitness to drive. Your answers have significant implications on your safety and the safety of others.
If you answer "yes" to any question, provide a detailed explanation as requested. Attach additional sheets of paper if the space provided is insufficient to explain your condition comprehensively.
Contact your physician if you are unsure about how to answer a specific question. Your health care provider can offer valuable insights into how your medical conditions might affect your driving capabilities.
Verify that your physician completes their portion of the form, if applicable. Their confirmation and additional details about your health condition are critical components of the assessment process.
Review your answers and ensure that all information is accurate and complete before signing the form. Your signature attests to the truthfulness and accuracy of the information provided.
Things You Shouldn't Do:
Don't leave any questions unanswered. Incomplete forms can delay the processing time or result in the rejection of your application.
Avoid guessing answers. If you are uncertain about a question, it's better to seek clarification from a health care professional than to risk providing incorrect information.
Don't use this form for commercial licensing requirements. The DL 546 form is designed for non-commercial drivers. Commercial drivers have different forms and medical prerequisites.
Refrain from withholding information about your medical condition. Failure to disclose relevant health issues can lead to serious legal and safety consequences.
Don't forget to give your consent for the release of medical information. Your signature and the physician's details are necessary for the DMV to verify the information, if needed.
Avoid submitting the form without reviewing it for accuracy. Typos, incorrect dates, or unclear handwriting can affect the DMV's ability to process your form.
Properly filling out the DL 546 form is a key step in ensuring that all drivers on the road are capable and healthy enough to operate a vehicle safely. By following these guidelines, you're not just complying with regulations, but you're also contributing to the overall safety and wellbeing of everyone on the road.
Misconceptions
There are several misconceptions about the California DMV DL 546 form, which is a Health Questionnaire required by the Department of Motor Vehicles. Understanding these misunderstandings can help ensure that individuals complete and submit the form accurately and according to the requirements.
- Misconception 1: The form is only for drivers with existing medical conditions. Some may think the DL 546 form is exclusively for those who have known medical disabilities or conditions. However, this form is a broad assessment meant to identify any health issues that could impact a person's ability to drive safely. It applies to all applicants who are asked by the DMV to complete it, not just those with known conditions.
- Misconception 2: Personal information is shared widely. There's a common concern about the privacy of the information provided on the DL 546 form. The details filled out on this questionnaire are used by the DMV to assess driving capabilities and are protected under privacy laws. The DMV does not share personal health information freely; access is restricted to authorized personnel.
- Misconception 3: A “yes” answer automatically disqualifies you from getting a license. Another misunderstanding is that answering “yes” to any of the health questions will lead to an immediate disqualification from obtaining or retaining a driver's license. In reality, a “yes” answer requires further explanation and possibly a review by the DMV’s medical review team, but it doesn't outright disqualify an applicant. Each case is assessed individually, considering the details provided and additional medical information if required.
- Misconception 4: The form doesn't need to be updated unless conditions change. Many believe once they've submitted a DL 546 form, they don't need to resubmit or update their information unless their medical condition changes. However, the DMV requires that this form be submitted every two years, regardless of changes to an individual's health status. This regular update ensures that the DMV has the most current information regarding an individual’s health and ability to drive safely.
Understanding these misconceptions can help individuals approach the DL 546 form more effectively, ensuring they provide accurate and complete information to the California DMV. It's about maintaining safety on the road by assessing and managing health-related risks among drivers.
Key takeaways
When dealing with the California DMV DL 546 form, it's important to understand several key points that will guide you through the process of correctly completing and submitting the form. The following takeaways aim to make this process clearer for drivers in California:
- Specific Purpose: The DL 546 form is designed exclusively for non-commercial drivers to report their health status. It is vital to the assessment of a person's medical ability to safely operate a motor vehicle.
- Importance of Accuracy: Applicants must answer every question truthfully, ensuring their responses accurately reflect their current medical condition. Incorrect or misleading information can have serious consequences.
- Physician Consultation: If unsure how to respond to a question, consulting with a healthcare provider is recommended. This can help ensure that the information provided is accurate and that any necessary explanations are clear and comprehensive.
- Explanation of "Yes" Responses: Any question answered with "Yes" requires a detailed explanation. This can be done in the space provided or on a separate piece of paper, which should be attached to the form upon submission.
- Frequency of Submission: The DL 546 form must be completed and submitted every two years. This regular update helps the DMV assess any changes in a driver's health status that might affect their driving abilities.
- Role of the DMV: Based on the responses and explanations provided, the DMV may contact the applicant's physician to further assess the driver's medical qualifications. This step is crucial in determining whether any health conditions could impair driving ability.
- Consent for Release of Medical Information: By signing the form, drivers consent to the release of their medical information by their physician to the DMV. This consent is necessary for the DMV to verify the health information provided and ensure public safety on the roads.
- No Commercial Use: It is crucial to note that the DL 546 form is not applicable for commercial licensing requirements. Individuals seeking or holding commercial driver's licenses (CDLs) must adhere to different procedures and forms specific to commercial driving.
Understanding these key aspects of the California DMV DL 546 form is essential for drivers to ensure they meet the state's requirements for holding a driver's license. Accurate and truthful completion of the form supports the DMV's goal of maintaining safe roadways for all users.
Different PDF Templates
California Department of Health Care Services - Details concerning significant business transactions with Medi-Cal are required to ensure transparency in the provider's operations and financial dealings.
Form 540 Instructions 2023 - Navigate the intricacies of converting federal adjustments to fit California's tax framework with Schedule CA (540) detailed guidance.